by Joe Maher, CPA, MBA
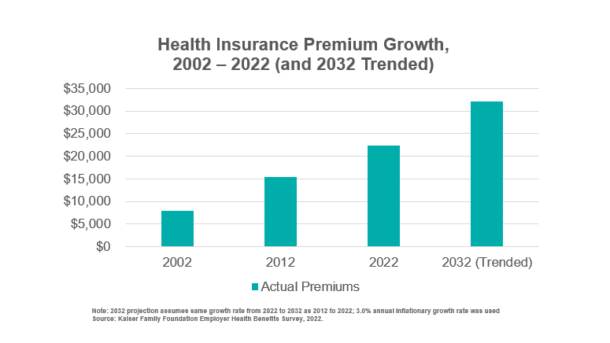
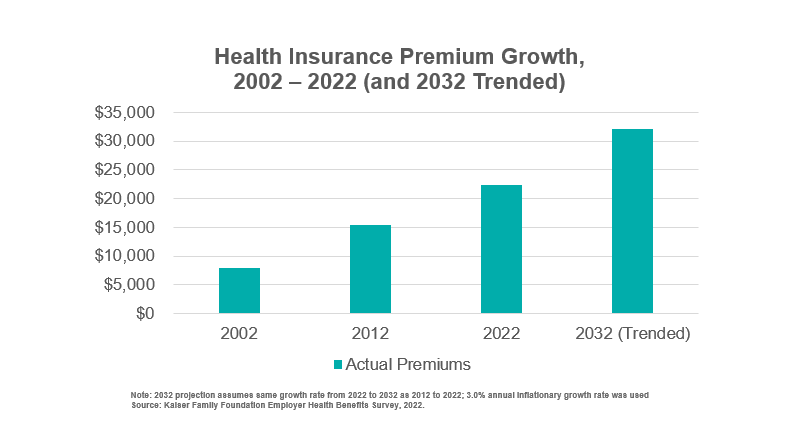
Many health systems have explored direct-to-employer opportunities at some level in recent years, but there needs to be more traction to show for these efforts. It is no secret that employer-funded commercial health insurance has provided the financial margin for providers, payers, benefits advisers and others in the ecosystem. Despite offerings from new entrants and incumbents designed to help employers reduce healthcare spending, these expenditures continue to significantly outpace inflationary costs.
Health systems and providers are seeing continued growth in the public payer mix driven by the aging population and expanded access to Medicaid. Within the decade, average health insurance premiums for private insurance family coverage are on pace to exceed $30,000 annually. It will be difficult for employers to bear that level of spending growth without taking more substantial action.
Despite significant financial incentives to approach healthcare spending differently, there are multiple reasons why the status quo persists. Employer health spending is embedded in a complex ecosystem with numerous key stakeholders coupled with significant information asymmetry.
- Employers are risk-bearing entities in almost all cases, either directly through self-funded plans or indirectly through insured plans. Despite responsibility for covering costs, there is rarely commensurate expertise internally. Consequently, it often gets delegated to human resource (HR) teams with broad responsibilities. Implementing benefit changes also falls to HR, so there is an understandable aversion to making changes. Even when facing year-over-year cost increases, the path of least resistance is to begrudgingly cover the cost increase.
- When employers do make changes to employee benefits, there is almost always some resistance from employees. Even small changes require implementation support in enrollment and onboarding. More significant changes require more hands-on navigation. Beyond the additional time and resource demands, HR often receives a vocal subset of employees who are unhappy with the benefit modifications. This can create a lot of noise and distraction. However, company leaders, especially in HR, know well that benefit changes designed to target healthcare costs will be met with some level of dissatisfaction.
- Advisers (agents, consultants, brokers) usually favor the status quo. They function as trusted partners for employers, given their subject matter expertise and resourcefulness, so most employers lean heavily on their guidance. In line with the reasons outlined for HR above, advisers also prefer incremental changes because it places less time burden on their constituents (both leadership and employees). When more significant changes to employee benefits are made, these advisers also need to spend more time supporting implementation.
- Meaningful change requires a multi-year horizon. Benefit selection cycles usually move in one-year increments, and for larger employers, the process starts many months before any roll-out. On top of that, value-based care business models typically take a few years to bend the cost curve effectively. At the point employers are willing to make dramatic changes, this multi-year horizon is usually less attractive than a plan change that cuts costs for the next year (and budget cycle), even if it does not do anything to reposition the organization for lower costs over the long-term sustainably.
Understanding these equilibrium forces can help health systems better position themselves strategically for engaging with employers. While the horizon for when employers will reach a tipping point on health spending may need to be clarified, health systems that can further invest in these relationships are better positioned to differentiate from local employers. Having strong, trusted relationships can help health systems earn a spot at the table as a partner with a solution rather than risk being viewed as a contributor to the problem. Health systems and providers can uniquely bring scale and resources that connect capabilities in service of a more integrated approach to employee health and cost containment.
Fortunately, some health systems have effectively engaged with local employers. When we look to these systems for best practices, a few key learnings stand out:
- Bring a differentiated value proposition that builds on core strengths and capabilities while resonating with the goals of the employer community (especially bending the cost curve).
- Recognize employer engagement opportunities can extend beyond bundles, on-site clinics and preferred network arrangements. These include wellness programs, health fairs and screenings, and integrated occupational health offerings.
- Take the long view by meeting employers where they are and build on the relationships over time.
- Dedicate internal resources to relationship building, business development and account management. Align these resources within the health system’s organizational structure to ensure they are positioned to be effective.
- Understand the role and incentives of all the key stakeholders involved in decision making.
Employer healthcare goals align closely with the Triple Aim goals of better health outcomes, improved patient experience and lower healthcare costs. Addressing the cost aim is critical to meaningful engagement and scalable solutions. Organizations with a more robust value-based care infrastructure are better positioned to partner with employers and drive transformative change.
No matter where your organization stands on its journey to engaging with employers and integrating value-based care, our experts are equipped to provide unique insights and impactful recommendations in prioritizing opportunities and positioning your organization for select value-based care undertakings. Learn more about Vizient’s Direct-to-Employer Healthcare Solutions and reach out to speak with a value-based care expert.
Related resources:
- Share