by Gregg A. Masters, MPH
In a sea of relentless ‘acronym soup’ that peppers the landscape and too often separates us from the constituency we ostensibly serve (patients) via added layers of dubious complexity to the dysfunctional  U.S. healthcare delivery and financing ecosystem, the Centers for Medicare and Medicaid Innovation (CMMI) has added the ‘‘ to our expanding nomenclature.
U.S. healthcare delivery and financing ecosystem, the Centers for Medicare and Medicaid Innovation (CMMI) has added the ‘‘ to our expanding nomenclature.
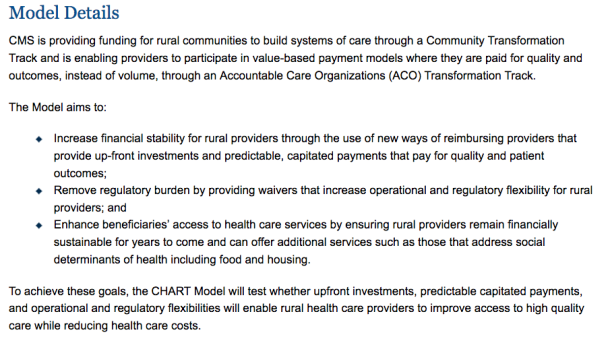
While we work through and perhaps finally remedy chronic and historically prevailing health in-equities across both urban and sub-urban settings vs. that typically found in rural markets driven by a ‘book of business’ (or financial class) series of incentives, the CHART model:
…aims to continue addressing disparities by providing a way for rural communities to transform their health care delivery systems by leveraging innovative financial arrangements as well as operational and regulatory flexibilities.
No doubt a noble cause and the ‘innovators’ at CMMI are to be recognized and commended for their efforts to make a meaningful difference in the lives of American’s who do not benefit from the typical healthcare asset concentrations in major markets – primarily urban and sub-urban.
While the range of ACO models – both commercial and public sector, i.e., Medicare and Medicaid – are seen by many as tepid responses to an uncharacteristically change or reform resistant healthcare economy fueled principally by still prevailing fee-for-service production incentives, we’re still early on in the evolution of this managed competition model of healthcare innovation, i.e., the ‘efficacy’ jury of ACOs to deliver on the ‘triple aim’ in aggregate is still out.
So read on and see what you think about the prospects of the CHART model to materially impact healthcare delivery while adding value to restraining the cost basis for accessing essential health services for largely under-served communities.
As always, your thoughts and comments are welcome.
==##==